Disclaimer: Early release articles are not considered as final versions. Any changes will be reflected in the online version in the month the article is officially released.
Author affiliations: Texas Department of State Health Services, Austin, Texas, USA (T. Sidwa, R. Traxler, E. Swaney, B.J. O’Sullivan, K. Parker); Centers for Disease Control and Prevention, Atlanta, Georgia, USA (J.S. Salzer, W.A. Bower, K. Hendricks); Shannon Health System, Ozona, Texas, USA (M.L. Sims); Shannon Medical Center, San Angelo, Texas, USA (P. Bradshaw); Texas Department of State Health Services, El Paso, Texas, USA (K.A. Waldrup)
The zoonotic disease anthrax, caused by the bacterium Bacillus anthracis, has been known to humankind for thousands of years and is endemic to most continents (1–3). It is a naturally occurring disease of herbivores that incidentally infects humans through contact with animals that are ill or have died from anthrax or through contact with B. anthracis–contaminated byproducts such as meat, hides, hair, and wool (4). Transmission routes include cutaneous, ingestion, inhalation, and injection; cutaneous accounts for most (95%) cases worldwide (2,4). In the United States, human risk is primarily associated with handling carcasses of hoofstock that have died of anthrax; the primary risk for herbivores is ingestion of B. anthracis spores that can persist in suitable alkaline soils in a corridor from Texas through Colorado, the Dakotas, and Montana (5–7).
Figure 1
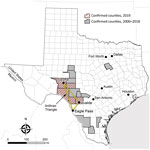
Figure 1. Counties with confirmed animal anthrax cases, Texas, USA, 2000–2019. The location of the “Anthrax Triangle” is indicated.
The 2 state agencies responsible for anthrax surveillance in Texas are the Texas Department of State Health Services (DSHS) and the Texas Animal Health Commission (TAHC). Samples that are culture-positive for B. anthracis at veterinary reference laboratories are reported to DSHS and TAHC. Veterinarians treating animals with illnesses compatible with anthrax might also contact DSHS or TAHC. Suspected cases of human anthrax are immediately reportable to DSHS. Samples or isolates from human cases are forwarded for identification to local public health reference laboratories. In Texas, animal anthrax cases are most commonly reported from the triangular area bounded by the towns of Uvalde, Ozona, and Eagle Pass (Figure 1), which includes portions of Crockett, Val Verde, Sutton, Edwards, Kinney, Uvalde, Zavala, and Maverick Counties in southwestern Texas.
During 2000–2018, a total 63 animal anthrax cases were confirmed by culture of B. anthracis in a reference laboratory (annual mean 3.3, range 0–20 cases/year) (T. Sidwa, unpub. data). Because only 1 animal per premise usually is reported each year, the number of cases is a substantial underrepresention of the total number of affected animals and properties. The last naturally occurring human case of cutaneous anthrax associated with livestock exposure in Texas was reported in 2001 (8,9).
Texas Outbreak 2019
Animal Cases
Texas Veterinary Medical Diagnostic Laboratory confirmed the first anthrax case of 2019 in an exotic antelope carcass from Uvalde County on June 19. Overall in 2019, the laboratory reported 25 culture-positive animals, including cattle, horses, white-tailed deer, antelope, and a goat, from Crockett, Kinney, Sutton, Uvalde, and Val Verde counties. The last confirmed animal case was reported on August 21. Unconfirmed numbers reported to DSHS staff suggest that >1,000 animal losses might be attributed to the 2019 outbreak (K. Waldrup, unpub. data).
Implementing control measures (i.e., vaccination and proper carcass disposal) was challenging; thin topsoil over bedrock, vast and inaccessible terrain, and burn bans triggered by hot, dry weather conditions made it difficult for livestock owners and landowners to identify and bury or burn dead animals. Livestock owners can sometimes cover dead animals with tarps if burial or burning is not an option. However, because properties in this area of Texas can be thousands of acres and not particularly navigable, reaching dead animals to cover and protect them from scavengers (that might further distribute B. anthracis–contaminated remains) is often not feasible.
Another obstacle to controlling the outbreak was the inability to address the contribution of wildlife to the initiation and perpetuation of disease spread (e.g., lack of a licensed vaccine and impracticality of using physical or chemical restraint to administer vaccine “off label” to wildlife species). In addition, reports of vaccine-associated adverse events among goats and horses (2,10) made some owners reluctant to vaccinate these species. Among confirmed animal anthrax cases in species for which vaccination is indicated (cattle, goats, horses, sheep, and swine) (11), a third are reported to have been vaccinated before illness. Of those, the median number of days from most recent vaccination to specimen collection was 8 days (range 3–82 days) (T. Sidwa, unpub. data). The frequency and effect of antibiotic use subsequent or simultaneous to vaccination was unknown.
Human Case Report
On July 23, 2019, a non-Hispanic White man in his 70s from the anthrax-affected area who had a history of cardiovascular disease and hypertension visited his physician for evaluation of 2 lesions near his right knee. Four days earlier, a small red spot had emerged and gradually enlarged and became painful. He reported no fever and used no over-the-counter medications. When asked about animal exposures because of where he lived, he reported that he and his daughter had moved 2 fly-covered deer carcasses from beneath his porch before lesion onset. He was wearing shorts and a shirt while moving the carcasses, and his affected leg was scraped by the velvet-covered antlers. He also reported being bitten by a fly. The deer carcasses were not tested for anthrax, and the patient disposed of them.
Figure 2
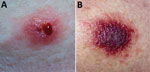
Figure 2. Lesions on right leg of anthrax patient as seen on outpatient visit, Texas, USA, 2019.
On examination at his physician’s office, the patient’s vital signs were as follows: blood pressure 177/87 mm Hg; heart rate 76 beats/min; and temperature 98.3°F. Below and lateral to his right knee was an indurated, raised, erythematous 5-cm lesion with small ulcerations that oozed serosanguinous fluid and was surrounded by a blanched halo. Just proximal to his right knee was a nonindurated erythematous macule (Figure 2). No popliteal or inguinal adenopathy was present. After 2 swab specimens were obtained from the larger lesion, the patient was given a cephalosporin intramuscularly, and a prescription for ciprofloxacin was called in to his pharmacy of choice more than an hour’s drive from his home. Because it was too late to send the specimens anywhere on that day, the swabs were mailed directly to the Texas Department of State Health Services Laboratory on Wednesday after a phone consultation with the state health department.
Figure 3

Figure 3. Bacillus anthracis24-hour growth on sheep blood agar from a swab of a cutaneous anthrax lesion from a patient in Texas, USA, 2019. Typical ground glass colony morphology and lack...
Figure 4
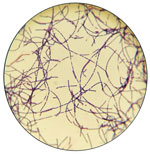
Figure 4. Gram stain from culture of a lesion of an anthrax patient, Texas, USA, 2019.
The patient began his ciprofloxacin the next evening (July 24). On July 26, after having taken 4 doses of his antibiotics, he was feeling worse and sought additional care at the emergency department of hospital A, more than an hour’s drive from his residence. Concurrently, the state laboratory notified his primary-care physician that a preliminary laboratory report for the specimen was PCR-positive for B. anthracis; this result was confirmed by culture the following week (August 1) (Figures 3, 4). His physician relayed the information first to the patient and then to hospital staff. Upon arrival to the hospital, the patient reported pain, difficulty walking, and nausea. He reported intermittent spontaneous drainage of a dark, jelly-like material from the larger wound. He reported no fever, chills, chest pain, shortness of breath, pain at rest, numbness, or tingling. He did not use tobacco products.
Figure 5
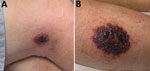
Figure 5. Eschars on right leg of anthrax patient as seen at hospital admission, Texas, USA, 2019.
At hospital A, he reported that his exposure had been »3 weeks earlier. At examination, his vital signs were blood pressure 132/71 mm Hg; heart rate 91 beats/min; and respirations 24 breaths/min. He was afebrile. He had a nondraining, nonerythematous eschar 7.2 cm × 5 cm on the lateral aspect of the right calf and a painless, nondraining, nonerythematous 3.3 cm × 2 cm eschar on the lateral aspect of the right knee (Figure 5). His leukocyte count was 12,000 (103 cells/µL); hemoglobin, 15.5 g/dL; hematocrit, 46.9% g/dL; platelets, 83,000 (103 cells/mL); blood urea nitrogen, 35 mg/dL; and creatinine, 2.6 mg/dL. His antibiotic was switched to intravenous doxycycline (100 mg every 12 hours). He was discharged on hospital day 13.
Control and Prevention Measures
Control Measures for Animal Outbreaks
Because naturally occurring human anthrax cases in endemic countries are almost always related to exposure to infected animals or their byproducts, control of animal anthrax essentially eliminates human risk. The primary control measure for animal anthrax is annual preventive vaccination; however, once an outbreak occurs, other control measures include ring vaccination, proper carcass disposal to avoid further environmental contamination, and quarantine (i.e., limit animal movement from the affected and nearby properties, animal contact with anthrax-contaminated sites, and contact between affected and nonaffected herds) (9). On the basis of anecdotal reports and 1 small study, tabanid flies (e.g., deer and horse flies) might play a role in transmission; whether fly control is achievable or would be effective remains an open question (2,12,13).
The attenuated Sterne-strain of B. anthracis is used globally for vaccination among domestic livestock (14). Because the vaccine is live-attenuated, concurrent antibiotic administration can substantially diminish efficacy. If an animal is given antibiotics either 10 days before or after vaccination, revaccination is recommended (9,15). Whether concurrent administration of antibiotics played a role in diminished vaccine efficacy in the Texas outbreak is unclear.
Proper and safe carcass disposal is critical for controlling anthrax outbreaks in enzootic areas because inappropriate carcass disposal seeds the soil with spores and increases the risk for future epizootics. Global recommendations (9) and codified Texas regulations (16) for carcass disposal are similar: the carcass should be burned in place, using a pyre or other method that leaves only ash and allows the destruction of the contaminated soil as well (i.e., “burnt until it is thoroughly consumed”) (9,16). When a carcass cannot be burned, global recommendations are to bury it deeply (9). The historic practice of adding lime should be avoided (17). High soil calcium levels, either from the addition of lime or as occur naturally in southwest Texas, are conducive to B. anthracis spore survival (6,7) and increase the likelihood of future outbreaks. The least desirable disposal method is leaving the carcass in place, because scavenging can further disseminate the spores and increase future exposure risks for susceptible animals. Alternative carcass disposal methods are needed in areas where the standard recommendations to burn or bury carcasses are impractical. This need is particularly pronounced where there is an abundance of susceptible wildlife species that are not vaccinated or where there is poor vaccination coverage of domestic hoofstock.
Prevention of Human Cases in Endemic Areas
Human and animal health authorities should remind at-risk populations of the following prevention measures when animal cases are first identified. During animal outbreaks of anthrax, persons who handle and dispose of infected animals are at highest risk for exposure. However, exposure can be minimized through use of personal protective equipment, which should include gloves that can be disinfected or disposed of, long sleeves and pants, and footwear suitable to the terrain that can be disinfected (9). Even in the absence of a recognized anthrax outbreak, veterinarians and ranchers in endemic areas should always keep anthrax in mind as they interact with members of susceptible species that are ill. To do otherwise can result in inadvertent exposure to anthrax.
Antibiotic postexposure prophylaxis (PEP) is another important component of prevention. In the former Soviet Union, before 1965, 58/339 (17%) of patients who did not receive antibiotic prophylaxis after cutaneous exposures had onset of anthrax; in contrast, only 5/287 (2%) who received prophylaxis had onset of anthrax (18).
If skin or mucus membrane contact occurs during carcass disposal, persons should seek medical attention and receive antibiotic PEP for 7 days (Table 1) and have their symptoms monitored for 14 days. Although aerosol exposure is unlikely in cases of natural cutaneous exposures, if potential aerosol exposure also occurred, antibiotic PEP should be administered for up to 60 days and anthrax vaccine may be considered.
Persons who live and work in anthrax-endemic areas and who anticipate interacting with animals that are dying or have died of anthrax might wish to consider preexposure prophylaxis with anthrax vaccine adsorbed (AVA). For preexposure prophylaxis of persons at high risk for B. anthracis exposure, AVA is administered intramuscularly as a priming series at 0, 1, and 6 months, with booster doses at 12 and 18 months and annually thereafter (19). Regional health departments in endemic areas that have existing vaccination programs can acquire AVA from the manufacturer.
Healthcare Infection Control Issues for Cutaneous Anthrax
A person with cutaneous or other type of anthrax (e.g., injection, ingestion, or inhalation) cannot transmit disease through aerosol or droplet. However, spores that could remain on a person’s skin, hair, or clothing after an exposure before they bathe or shower and change clothes might possibly transfer to someone else’s skin and cause cutaneous anthrax (20–22). Although incubation periods of <1 day are reported, patients usually wait a few days to seek care, making it likely that they would already have bathed and changed clothes. It is therefore unlikely that healthcare personnel would be secondarily exposed to spores.
Although cutaneous anthrax lesions can be contagious before the institution of effective antibiotic therapy, they become sterile in <1 day once therapy has begun (23). Lesions should be covered until the patient has had 24 hours of effective antibiotics. Contact precautions should be used for the first day; after that, standard precautions are sufficient.
Disposable items that have been in direct contact with the anthrax lesion, any tissue removed during debridement, and potentially infectious wound care materials (24,25) should be disposed of in a biohazard bag according to guidelines for disposal of any potentially infectious material. No additional disinfection is needed beyond what is regularly scheduled for the facility. Nondisposable surfaces in direct contact with the anthrax lesion or wound drainage can be disinfected with a 0.5% hypochlorite solution, a commercial product such as SporGon (Decon Labs, https://deconlabs.com), or other sporicidal agents such as an Environmental Protection Agency–registered antimicrobial product effective against B. anthracis spores (26–28); products effective against Clostridium difficile spores might also be appropriate (29,30)
Diagnosis
Although an eschar is the cardinal sign of cutaneous anthrax, in its early stages, anthrax can manifest as a group of small vesicles that might be pruritic. The lesion might be surrounded by erythema and swelling but is usually painless. Lymphadenopathy can occur, and constitutional symptoms including fever and headache are also possible. Localized cutaneous anthrax can disseminate to become a systemic disease. Although a substantial portion (10%–40%) of patients with cutaneous anthrax would die if left untreated (4), most can recover with treatment (31). Meningitis is also a possible, and typically fatal, complication (32).
In the United States, cutaneous anthrax is decidedly rare: other causes of eschars and eschar-like lesions include poxvirus infections (e.g., cowpox, vaccinia, orf), rickettsial infections (e.g., scrub typhus and Rickettsia parkeri rickettsiosis), ulceroglandular tularemia, staphylococcal or streptococcal infections, and noninfectious causes such as insect or spider bites. Obtaining a good exposure history is key to determining the likelihood of various etiologies among the differential diagnoses and determining the best specimens to collect. Patients seeking care with an eschar or eschar-like lesion should be asked about recent exposure to dead or dying herbivores or biting flies in an anthrax enzootic area; recent animal bites or scratches; and recent contact with lagomorphs, rodents, fleas, ticks, and spiders.
A Gram stain of a swab specimen from the lesion can often quickly identify possible cases and narrow the differential diagnosis (23). Specimens for tests such as Gram stain, culture, and PCR to rule anthrax in or out (Table 2) must be collected before the use of antibiotic therapy because they will rapidly become negative after the implementation of therapy (23). Specimens can be sent to sentinel laboratories for preliminary assessment. Specimens for which B. anthracis is not ruled out by a sentinel laboratory should promptly be sent to a Laboratory Response Network (LRN) laboratory for confirmation (33). LRN is a network of laboratories established to respond to biologic and chemical threats and other public health emergencies that consists of 3 types of laboratories. Private and commercial laboratories comprise the first tier of the LRN and are described as sentinel laboratories. Laboratories that receive reagents, protocols, and specialized training to perform confirmatory testing for multiple agents in high-risk environmental or clinical samples comprise the second tier of LRN and are referred to as reference laboratories. Specialized characterization of organisms, bioforensics, select agent activity, and handling of highly infectious biologic agents is performed at national laboratories, the third tier of LRN. However, with approval from public health authorities, specimens from lesions that are highly suspicious based on clinical or epidemiologic grounds can be sent directly from clinicians to an LRN laboratory (34).
Notification
Clinicians should promptly notify their local or state health department when they suspect anthrax, although the mandated timing varies by jurisdiction. State and territorial health departments should notify the Centers for Disease Control and Prevention (CDC) within 4–24 hours (24) of the initial report for patients whose illness meets the probable or confirmed case definition (35). Presumptive positive results from an LRN laboratory must be reported within 2 hours to the state and CDC.
Treatment
Cutaneous anthrax lacking systemic manifestations such as fever, tachycardia, tachypnea, hypotension, leukocytosis, or leukopenia can usually be treated with 7 days of an oral antibiotic. Patients with cutaneous anthrax should only continue oral antibiotics for PEP after antibiotic treatment is complete if the patient was also exposed to aerosolized spores; this would rarely be indicated for naturally acquired cutaneous infections because aerosol exposures are unlikely (Table 1).
Systemically ill patients should be evaluated for meningitis; if meningitis can be ruled out, they should be treated with at least 2 intravenous antibiotics (1 that is bactericidal and 1 that inhibits protein synthesis to block toxin production). Antibiotic therapy should continue for >2 weeks or until the patient is stable. If meningitis is present, >3 antibiotics should be used (>1 should be bactericidal, >1 should inhibit protein synthesis, and all should have good central nervous system penetration). Antibiotic options for treatment and prevention of anthrax are listed in Tables 1 and 3.
Systemically ill patients (whether from cutaneous, ingestion, inhalation, or injection exposures) are candidates for 1 of the Food and Drug Administration–approved anthrax antitoxins. The antitoxins are available through the Strategic National Stockpile pending a consultation with an anthrax subject matter expert at CDC, which can be reached by calling the Emergency Operations Center (770-488-7100).
Surgery might occasionally be indicated for lesions complicated by compartment syndrome. However, surgery usually is not necessary for cutaneous anthrax (36).
Public Health Implications and Conclusion
Anthrax is endemic to parts of the United States. Epizootics emerge with varying frequency when climatic conditions favor the uncovering of soilborne B. anthracis spores with subsequent consumption by susceptible herbivores. Humans contract cutaneous anthrax through contact with animals that are ill or have died from anthrax or contact with B. anthracis–contaminated byproducts; this risk is increased during epizootics. The outbreak we describe was confirmed in June 2019, but its actual start date is unknown; reliable recognition of epizootics might be impeded when they occur in vast, rough, and sparsely populated areas such as those in the anthrax-endemic areas of Texas. These same geographic characteristics create challenges in implementing the recommended disease control interventions, including appropriate carcass disposal and broad use of animal anthrax vaccine in species for which the vaccine is licensed, as well as off-label use in other species. Wild herbivores (e.g., white-tailed deer and exotic hoofstock) contributed to the 2019 Texas outbreak, but effective mitigation (carcass disposal or vaccination) of the risk they posed could not be adequately achieved.
The cutaneous anthrax patient associated with this outbreak was apparently exposed through a scratch on the leg from the antler of an untested deer carcass. The physician he visited in rural Texas included anthrax in the differential diagnosis, obtained and submitted diagnostic samples before treating the patient, and provided the patient with a prescription for oral ciprofloxacin. Anthrax was identified through PCR and confirmed through culture at the state reference laboratory from swab specimens of a leg lesion. The patient was treated as an outpatient with appropriate antibiotics until his condition worsened and required a 13-day hospitalization. The necessity for hospitalization might have been related to a few-week delay in seeking treatment. Despite the delay, the patient, like most patients with cutaneous anthrax, survived with antibiotic treatment (4,32).
As soon as anthrax is recognized in an animal population, public health and animal health agencies must collaborate to heighten awareness among medical and animal health communities, as well as among ranchers and other inhabitants of at-risk areas. Timely delivery of information to ranchers on proper carcass disposal and appropriate use of personal protective equipment, as was done through various alerts, might reduce the number of exposures. If exposure is recognized, antibiotic PEP should be considered by medical providers. AVA may be appropriate for persons at high risk for exposure, such as veterinary staff and ranch workers in endemic areas; however, this process involves a long-term commitment to annual booster shots to ensure protection.
Ranchers and veterinarians should receive authoritative information on animal vaccine use to break the cycle of transmission (including emphasis on avoiding administration of antibiotics 10 days before or after vaccine administration). Even in the absence of a recognized anthrax outbreak, veterinarians and ranchers in endemic areas should keep anthrax in mind as they interact with ill members of susceptible species. Doing otherwise might result in inadvertent exposure to anthrax. A survey of ranchers in the outbreak area is planned by TAHC to assess knowledge, attitudes, and practices regarding anthrax, including information on livestock vaccination.
Recent federal anthrax guidance has focused on the treatment of systemic anthrax, including meningitis, rather than on the more common cutaneous form of the disease. Given that half the cases in the 2001 anthrax incident in the United States (37) were cutaneous anthrax and most sporadic cases in the United States and worldwide are cutaneous, this article provides an overview of prevention and control measures for animals and a single resource for the prevention, diagnosis, infection control, and treatment of naturally acquired cutaneous anthrax.
Dr. Sidwa worked for the Texas Department of State Health Services from 1993 to 2020 (retired January 31, 2020), most recently managing the Zoonosis Control Branch and serving as the State Public Health Veterinarian.
We thank Amanda Kieffer, Trevor Maness, Amanda Kammen, Kelly Persinger, Laura Robinson, Kelly Broussard, and Bonny Mayes for their assistance with this investigation and contributions to this article. We would also like to thank Thitipong Mongkolrattanothai for assistance with references and Mark Deka for preparing a map of the affected area.
This work is in memory of Robert “Dr. Bob” Dittmar, a friend, colleague, and Texas Parks and Wildlife Department (TPWD) State Wildlife Veterinarian who, along with 2 TPWD colleagues, was killed August 8, 2020, in a helicopter crash while conducting aerial surveys for desert bighorn sheep in TPWD’s Black Gap Wildlife Management Area. He will be missed.
Suggested citation for this article: Sidwa T, Salzer JS, Traxler R, Swaney E, Sims ML, Bradshaw P, et al. Control and prevention of anthrax, Texas, USA, 2019. Emerg Infect Dis. 2020 Dec [date cited]. https://doi.org/10.3201/eid2612.200470
The conclusions, findings, and opinions expressed by authors contributing to this journal do not necessarily reflect the official position of the U.S. Department of Health and Human Services, the Public Health Service, the Centers for Disease Control and Prevention, or the authors' affiliated institutions. Use of trade names is for identification only and does not imply endorsement by any of the groups named above.
"control" - Google News
November 13, 2020 at 01:42AM
https://ift.tt/3lvrGeI
Early Release - Control and Prevention of Anthrax, Texas, USA, 2019 - Volume 26, Number 12—December 2020 - Emerging Infectious Diseases journal - CDC
"control" - Google News
https://ift.tt/3bY2j0m
https://ift.tt/2KQD83I
Bagikan Berita Ini














0 Response to "Early Release - Control and Prevention of Anthrax, Texas, USA, 2019 - Volume 26, Number 12—December 2020 - Emerging Infectious Diseases journal - CDC"
Post a Comment